
Thousands of people are having to deal with mental health issues brought upon by the prolonged lockdown and other restrictions as the government tries to stop the spread of the COVID-19 virus. Wakini Njogu took a look at how community radio and tech tools are being used to provide psychosocial support and mental health services.
***
Amisa Rashid walks through the streets of Kibera with her ear to the ground. She runs a radio talk show on mental healthcare every Saturday from 11am for an hour on Pamoja FM, a community radio station. Each conversation that Amisa and her co-host Aisha Mohammed have on mental health is driven by different societal issues that Kibera residents are facing.
On the Saturday when I was within the three-kilometre radius served by Pamoja FM, I listened in. Amisa and Aisha were discussing the relationship between mental health and academic outcomes. Just days before, the Kenya Certificate of Primary Education (KCPE) exam results had been released. Given past reports of children committing suicide and parents disregarding their children’s education due to failing KCPE, Amisa knew that this was a hot topic.
Pertinent issues were raised. Parents treating children as retirement plans. Children who get good grades only so they can get validation from their parents, and how that might resort to them people-pleasing their way in life. And in a memorable call mid-conversation, a parent seeking to know how they can be involved in their children’s school lives, yet they never received any formal education.

Such engagements and reciprocal conversations with community members are what Amisa hoped for when she started the programme a year ago. The larger goal was to provide the community with an opportunity to openly discuss mental health issues that have previously been taboo. The talk show came in March 2020 at a much needed time, just when COVID-19 cases had been confirmed in Kenya. A counselling psychologist by profession, Amisa has been meeting the need for psychosocial support for hundreds of people, especially Kibera residents, who are suffering from the trauma, anxiety, and other mental health challenges brought on by the pandemic.
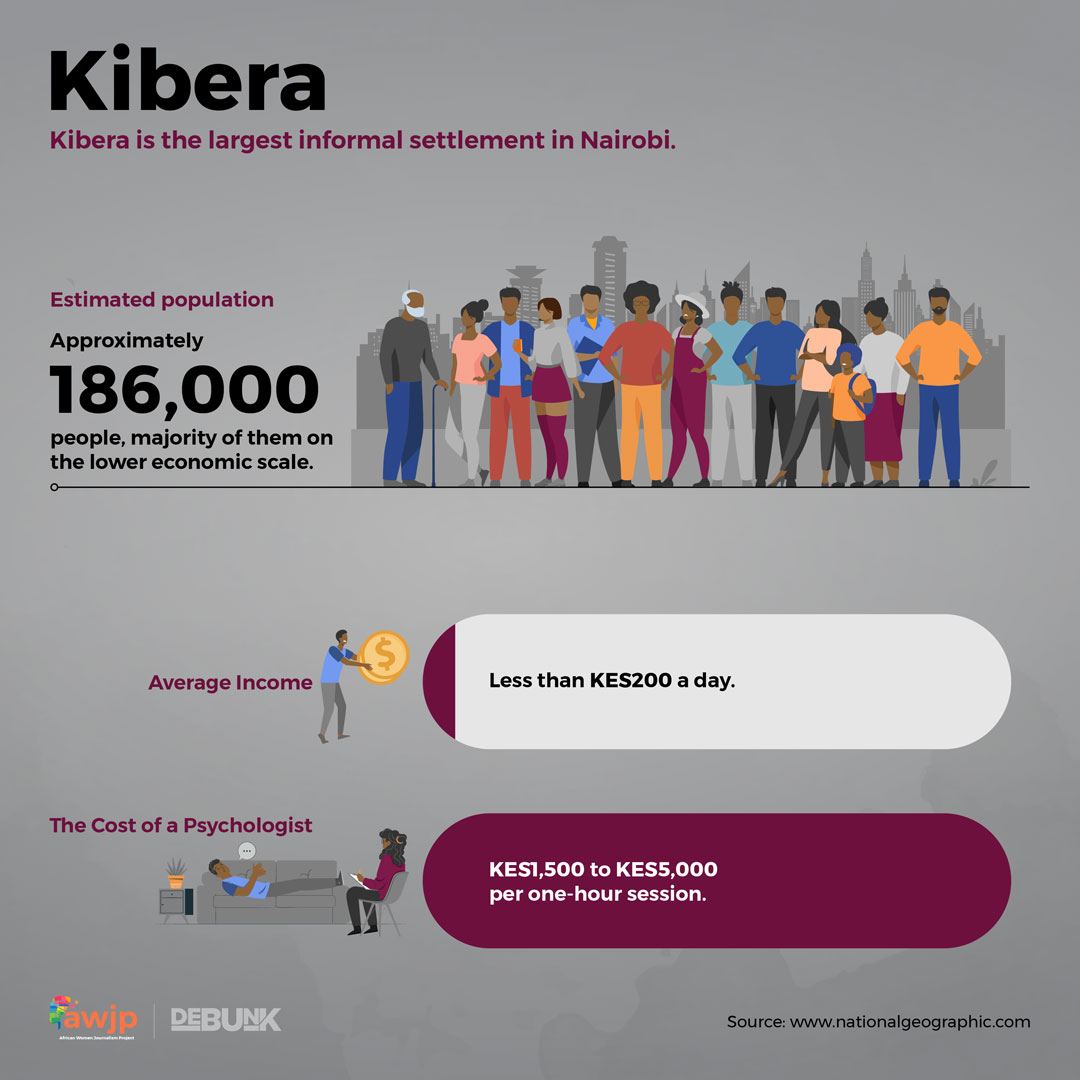
Kibera is the largest informal settlement in Nairobi with an estimated population of 186,000 people, the majority of them on the lower economic scale. Lack of financial stability often leads to poor mental health through social stresses and stigma and trauma.
Since 2018, Amisa has been working in Kibera to create awareness about mental health, and has been providing mental health services to the community through her organisation, Nivishe Foundation, whose objective is to build strong communities using mental health and trauma-informed resilience as tools for enhancing community cohesion.
The radio programme, hosted in Swahili, has gained popularity. “We have a listenership of about 10,000 people in the hour,” notes Amina gleefully. Listeners call in every week asking questions related to mental health. A common question that Amisa and her team often get is about schizophrenia, a mental health disorder that usually appears in late adolescence or early adulthood. Its impact on speech, thinking, emotions, and other areas of life can affect a person’s social interactions and everyday activities.
In the narrow streets of Kibera and elsewhere, there are numerous people suffering from mental health disorders who, because of their odd behaviour, are derided and shunned by the community. “These are the people you hear being referred to as wendawazimu (mad people),” says Amisa.
Whenever she is out on a walk in Kibera, she is often approached by different people, some of them simply thanking her for the programme and others inquiring how they can get further help for themselves or relatives suffering from mental disorders. It warms her heart that people have now started realising that the “wendawazimus” (a derogatory term for crazy people in swahili) in their families and community were ill and needed medical attention.
“Mental health stigma is going down,” Amisa opines. She further observes that the choice of words people use to describe mental health illnesses has also changed. More and more of her listeners are now able to attribute the “wendawazimu” to specific causes such as depression or stress to try and explain the bizarre behaviour of people suffering from mental diseases.
She recalls having a chat with a group of young people who initially thought that people who committed suicide were cursed. Through her radio show, the young boys were surprised to learn that suicidal thoughts are a sign of mental health illness and have nothing to do with curses. It is this kind of feedback that keeps her up at night wanting to do more.
“I look forward to Saturdays,” says Amina with a hint of joy and pride. Beyond this programme, Nivishe Foundation has incorporated sign language in their outreach to cater for community members with hearing impairment. The foundation also has an outreach programme targeting men, many of whom believe mental illness is ‘unmanly’ and therefore fail to recognise or even seek treatment.
There are 158 licensed radio stations in the country, 20 of which are community radio stations that have a broadcast radius limitation of between three kilometres and 50km. The radio stations broadcast in local languages including Sheng while others use a mix of different languages such as Kiswahili, English and the respective local language. Local radios are a cost-effective and impactful way to reach a significant proportion of the population and also raise awareness, reduce stigma about mental health issues. However, the challenge is finding the technical words and phrases which are not commonly used locally.
There is no direct translation of most of the common mental disorders such as depression, anxiety, stress. Instead, descriptive words are used for these illnesses which can sometimes lead to misunderstanding. For example, in Dholuo, there is no specific direct translation of the word ‘depression’, so descriptive words such as kuyo, kibaji, and parruok are used. Mental Health terms and diagnosis have a variety of meanings depending on context and can refer to sadness, anxiety and worry or thinking a lot respectively.
Amisa attributes her foundation’s mental health talk show’s success to having done comprehensive background research on their target audience. This gave them a clear picture of how to approach different aspects of mental health based on Kibera’s societal issues. “Each target audience has a different mental health need,” she says. Additionally, Amisa advises that there should be avenues for follow-ups after the radio talk show to create more impact, such as community gatherings and workshops.

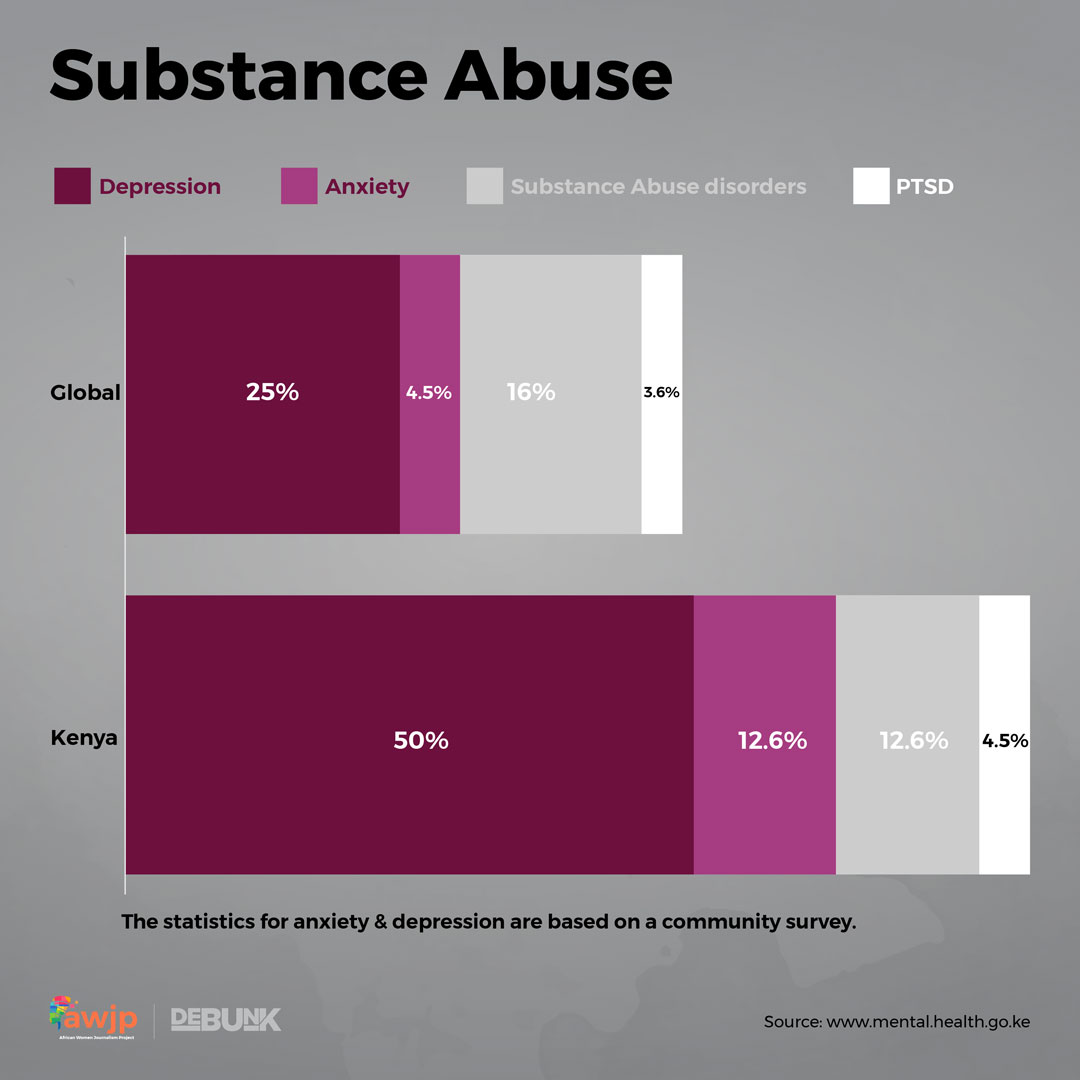
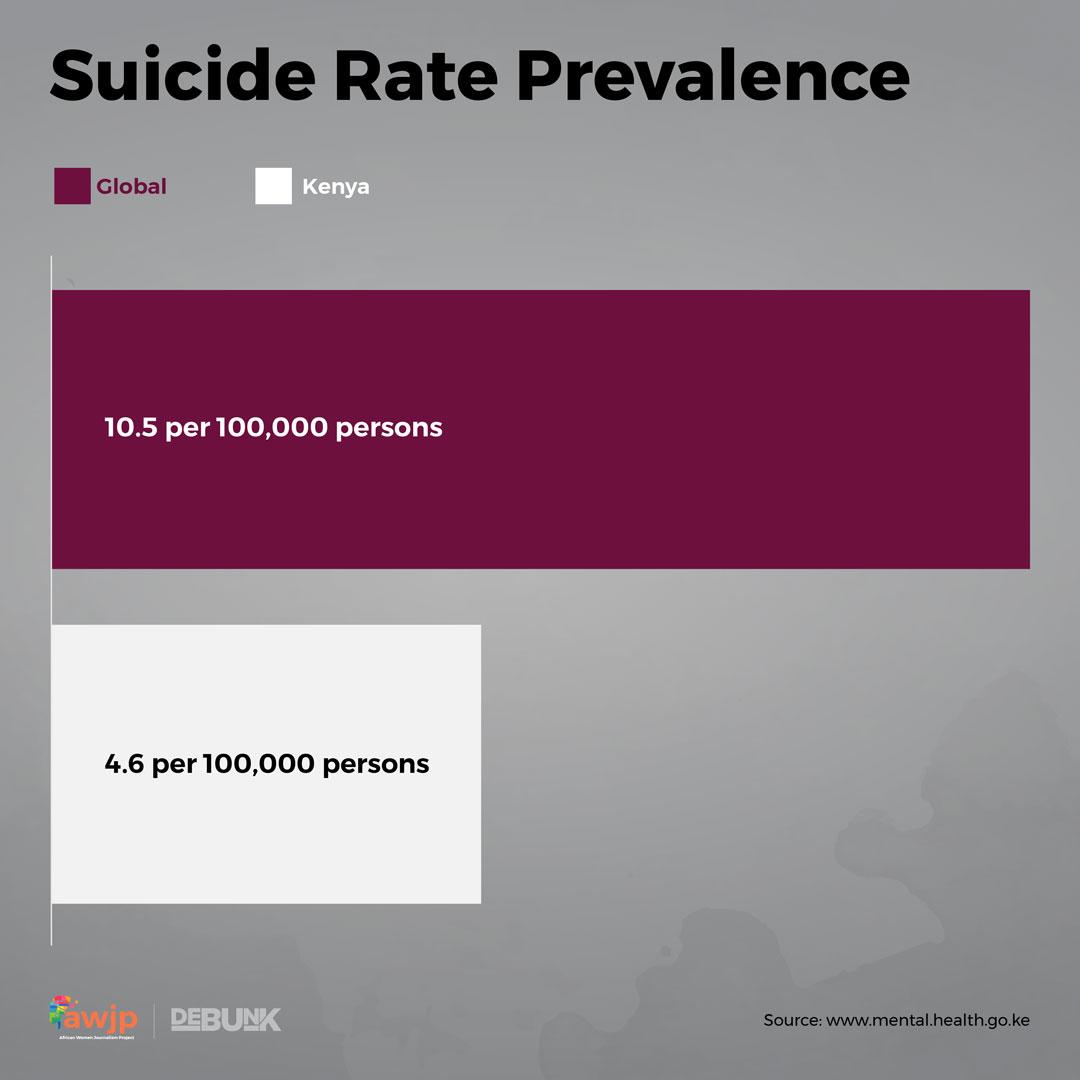
Globally, an estimated 792 million people suffer from mental health disorders. The largest number of people have an anxiety disorder, estimated at around 4 percent of the population. In Kenya, an estimated 1 percent of the population suffer from some form of mental illness with the most common mental illnesses being depression and suicide, substance use disorder, bipolar disorder, schizophrenia and other psychoses, according to the 2019 Kenya Population and Housing Census report.
The Task force on Mental Health report released in October last year found that “at least 25 percent of outpatients and 40 percent of inpatients in different health facilities had a mental illness, and an estimated prevalence of psychosis stated as 1 percent of the general population.”
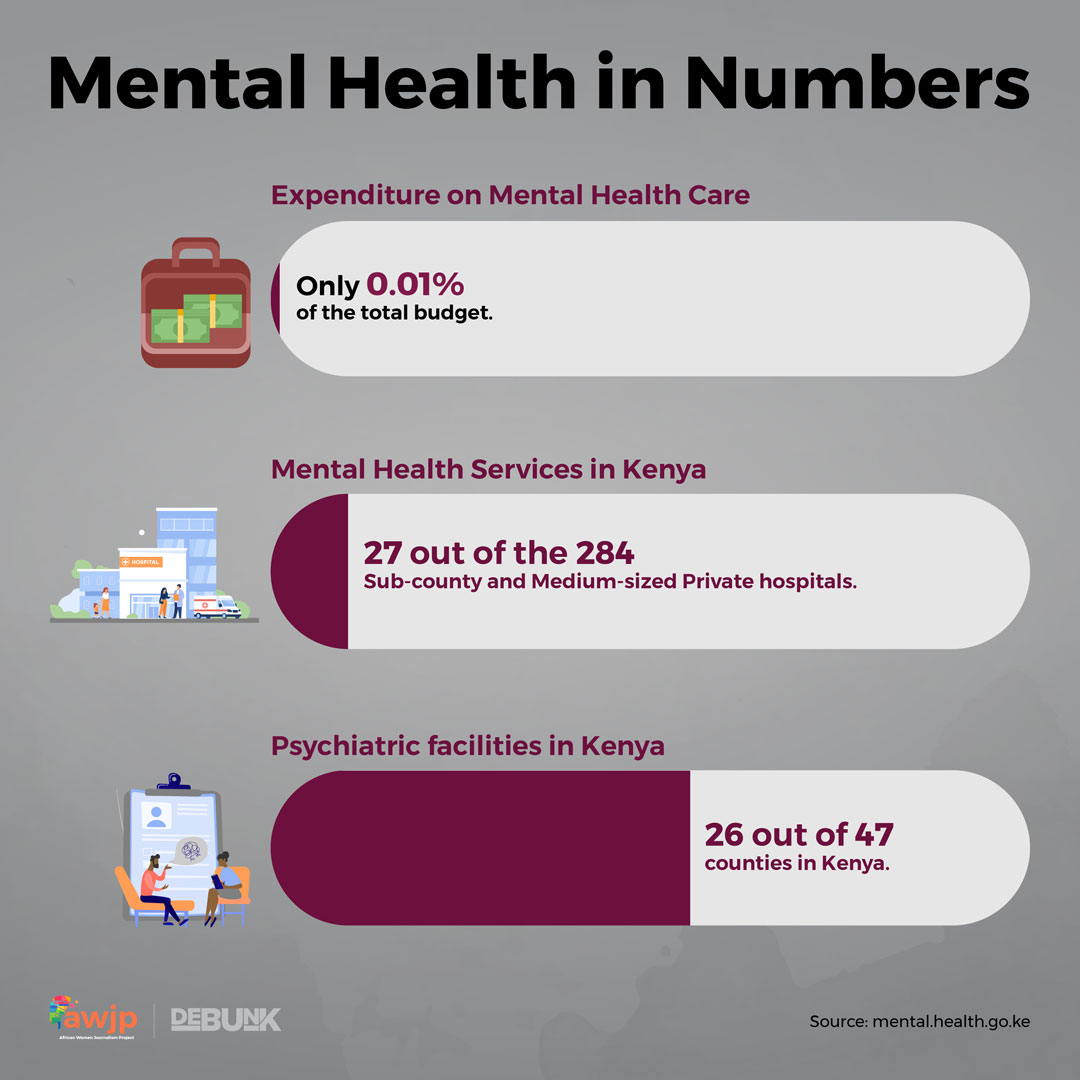
The systemic neglect in the provision of mental health services has been going on for years. The situation has not changed much since this report from 2011 from the Kenya National Commission on Human Rights. Spending on mental health is estimated at 0.01 percent of the total budget. Mental health services are only available in 29 out of the 284 Level 4 hospitals in the country, while psychiatric units are only available in 26 out of 47 counties in Kenya. This means that an estimated 75 percent of Kenyans are not able to access mental health services and rely on assistance from informal and community structures such as traditional healers, family, friends, and others. The cost of seeing a psychologist for a one-hour session mostly ranges from Sh1,500 to Sh5,000. This, for most Kenyans, especially with the looming economic crisis, is far out of their pockets’ reach.
Much like the Nivishe Foundation’s mission of improving communities’ mental health during the COVID-19 pandemic, Médecins Sans Frontières/Doctors Without Borders (MSF) launched a tech tool to help people deal with the anxieties caused by the pandemic. The MSF launched a chatbot that allows people in need of mental health tips to receive tailored advice to help them take action to deal with the emotions they are experiencing in a positive way. The chatbot was a simple yet effective means of reaching a wider audience.
MSF uncovered that the most common emotions people were likely to feel during the pandemic were sadness, anxiety, loneliness, fear, frustration, stress and negativity. This shaped the advice Nancy Nyambura, MSF’s psychologist, provided through the bot, including tips for helping people to cope with the reality of working from home.
“We want people to know that it is normal to have emotional reactions at a time like this,” says Nancy. “And by reading through other people’s stories, we hope people will feel that they are not alone, and will help them to cope better.”
Between June 2020 when it launched and December 2020, the Toolbox had an estimated 33,066 visits. The users include their staff working in humanitarian areas. And while the advice is free and available online, Nancy urges people who need more in-depth support to reach out to a psychologist or a counsellor near them for a more in-depth, one to one session.
While the Nivishe Foundation and MSF have created platforms to help mitigate the harmful impact of COVID-19 on the public’s mental health, the government has to do more to provide these tools and services to all Kenyans, and especially those living in the rural areas.
Indeed, at the very beginning of the pandemic, the COVID-19 response in Kenya had no formal plan to address mental health. Even though guidelines were developed for the management of mental health conditions, implementation was and is still a huge challenge due to a poorly resourced mental health system. While the government instituted surveillance for the disease, there has been no such surveillance instituted for mental health, even when there have been increased reports of substance addiction and suicide number.
Through the devolved health systems, county officials in charge of health should create mental health advocacy programmes tailored to each county’s context. For starters, the government should allocate more monetary and human resources to the provision of these services and implement a formal health response plan.
Community health volunteers and workers should be trained to provide basic psychological assistance to provide the support people need to deal with the anxieties and mental disorders caused by the pandemic.
And to collect up-to-date data to inform decision making, the county and national governments should introduce mental health indicators in the District Health Information System (DHIS2), the free and open-source health management data platform which is used to track disease incidences and vaccine delivery for immunisation programmes. The DHIS2 has been deployed for COVID-19 surveillance.
Further, the government should implement the Kenya Mental Health Policy which provides for a framework on interventions for securing mental health systems reforms. Kenya is one of the states that criminalises suicide attempts. Scarcity of data informing mental health decision-making is a big policy gap, and therefore funding research and data collection on the topic should be a top annual priority.
When mental health is left unattended by all stakeholders, it could lead to economic losses due to loss of productivity and reduced contribution to societal development. Leaders in different sectors should identify and address the social and economic factors that contribute to the onset and perpetuation of mental health disorders.
Months into the lockdown, the impact of the pandemic on mental health and the need to provide mental health services and support has not been, and is still not a priority.
It’s slightly over a year now since the mental health show debuted, and Amisa couldn’t be more proud. There has been nothing as refreshing as deconstructing stigma on the topic. Through Nivishe Foundation, they now have programmes in Kwale and Garissa, and as 2021 progresses, she hopes to expand her outreach to other counties.
This article was supported by the Africa Women Journalism Project (AWJP) in partnership with the International Center for Journalists (ICFJ).

